

Your basket is currently empty!
Anatomy – The Heart
Great Vessels of the Heart
Contents
The great vessels of the heart are responsible for transporting blood to and from the heart during the cardiac cycle. They are primarily situated within the middle mediastinum.
This article examines the anatomy and spatial relationships of the aorta, pulmonary arteries and veins, and the superior and inferior vena cavae.
Aorta
The aorta is the largest artery in the body and carries oxygen-rich blood from the left side of the heart to the systemic circulation.
It originates from the aortic orifice at the base of the left ventricle, with blood entering through the aortic valve. The initial portion is the ascending aorta, which lies within the pericardial sac and is covered by the visceral pericardium. The coronary arteries arise from this segment.
The ascending aorta continues as the arch of the aorta, from which the major arteries supplying the head, neck, and upper limbs originate:
- Brachiocephalic trunk
- Left common carotid artery
- Left subclavian artery
Beyond the arch, the vessel continues as the descending aorta, which travels inferiorly through the thorax and passes through the diaphragm to enter the abdomen.
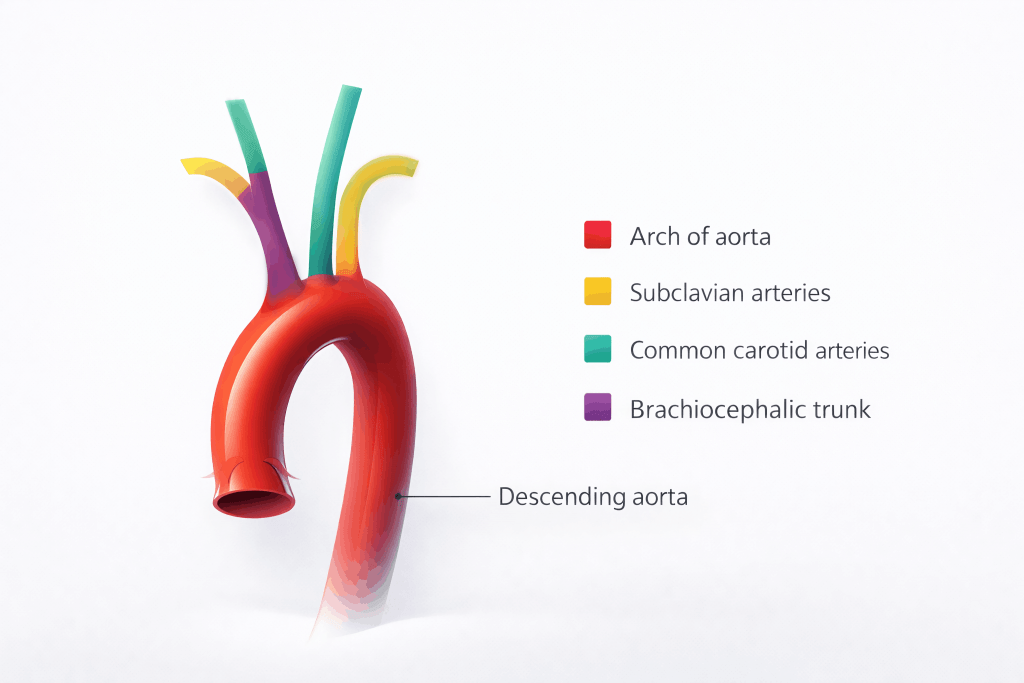
Fig 1 – The aortic arch and its relationship to the other great vessels.
Clinical Relevance
Disorders of the Aorta
Aortic Dissection
An aortic dissection occurs when a tear develops in the inner layer of the aortic wall. This allows blood to enter the wall of the vessel, creating a false channel alongside the normal lumen.
Blood within the vessel wall can compress the true lumen, reducing blood flow to distal tissues. It may also weaken the aortic wall, increasing the risk of dilation and aneurysm formation.
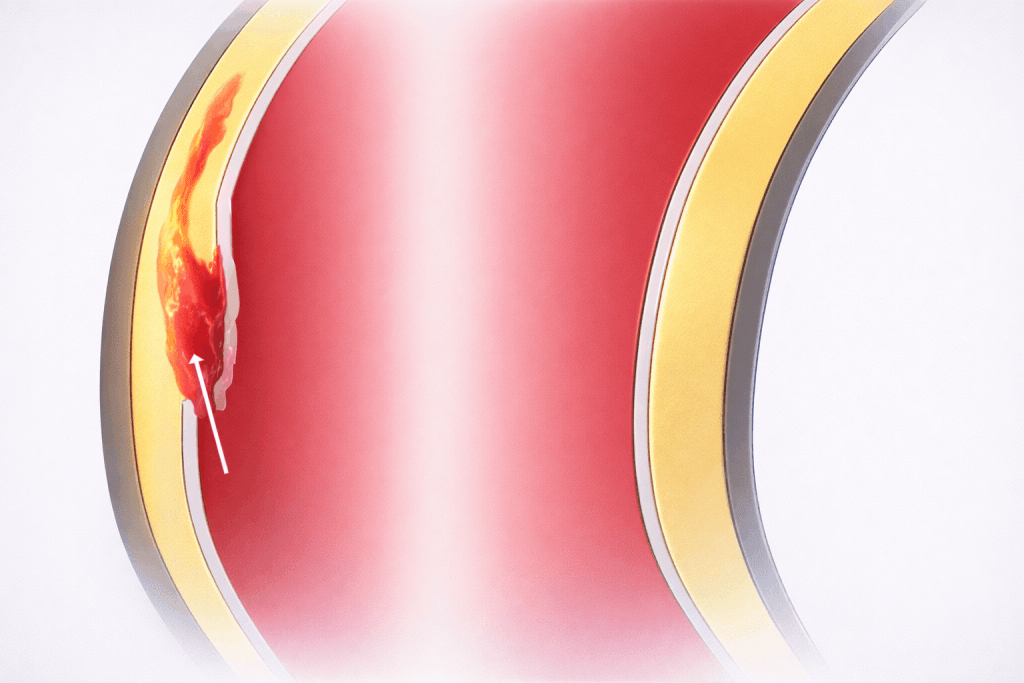
Fig 2 – Aortic dissection showing blood tracking into the aortic wall.
Aortic Aneurysm
An aneurysm is defined as a dilation of an artery exceeding 50% of its normal diameter. Aortic aneurysms arise due to structural weakness of the vessel wall, which may be congenital (such as in Marfan syndrome) or acquired (for example, following dissection).
The primary danger associated with an aortic aneurysm is rupture, which is frequently fatal if not treated promptly.
Pulmonary Arteries
The pulmonary arteries transport deoxygenated blood from the right ventricle to the lungs for gas exchange.
They originate as the pulmonary trunk, a short, wide vessel separated from the right ventricle by the pulmonary valve. The trunk lies anterior and medial to the right atrium and shares a common pericardial covering with the ascending aorta. It ascends, crossing in front of the aortic root before passing posteriorly.
At approximately the level of T5–T6, the pulmonary trunk divides into the right and left pulmonary arteries. The left pulmonary artery supplies the left lung and divides into two branches for each lobe. The right pulmonary artery is longer and larger, supplying the right lung and also dividing into two branches.
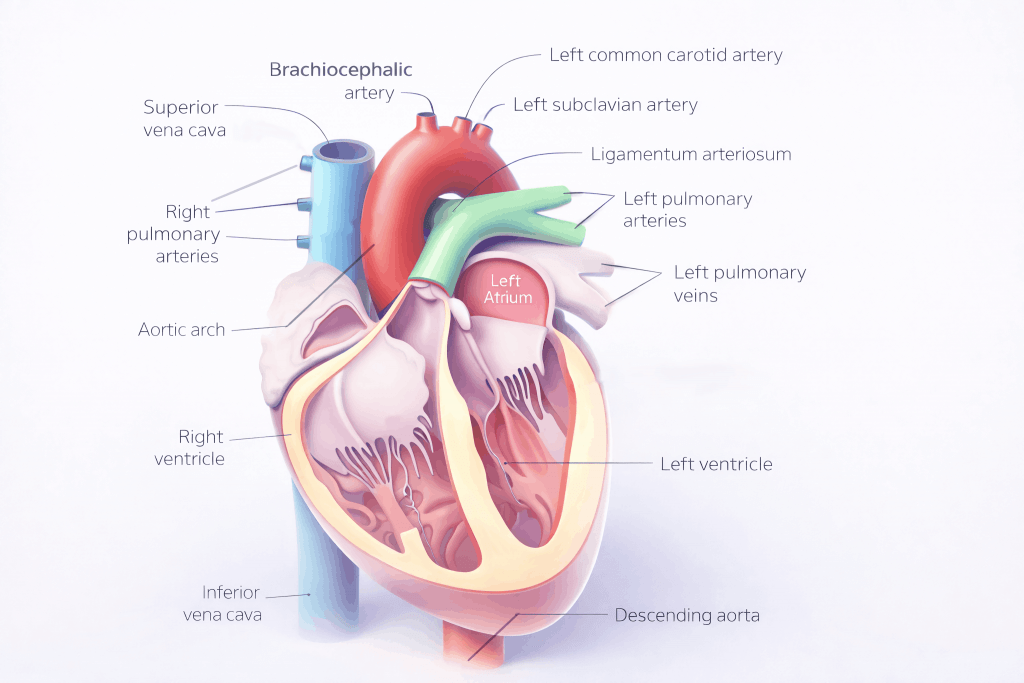
Fig 3 – Anterior view of the heart and its great vessels.
Pulmonary Veins
The pulmonary veins return oxygenated blood from the lungs to the left side of the heart for systemic circulation.
There are four pulmonary veins in total—one superior and one inferior from each lung. They enter the pericardium and drain into the posterior aspect of the left atrium. The oblique pericardial sinus lies within the pericardium between the left and right pulmonary veins.
The superior pulmonary veins drain blood from the upper lobes of the lungs, while the inferior pulmonary veins drain the lower lobes. The left inferior pulmonary vein lies at the lung hilum, whereas the right inferior pulmonary vein courses posterior to the superior vena cava and right atrium.
Superior Vena Cava
The superior vena cava returns deoxygenated blood from structures above the diaphragm—excluding the heart and lungs—to the right atrium.
It is formed by the union of the right and left brachiocephalic veins and descends through the thorax to enter the upper part of the right atrium at the level of the third rib.
During its course, the superior vena cava lies on the right side of the superior mediastinum before entering the middle mediastinum, where it runs adjacent to the ascending aorta.
Inferior Vena Cava
The inferior vena cava transports deoxygenated blood from the lower half of the body back to the heart.
It forms in the pelvis from the convergence of the common iliac veins and ascends through the abdomen, receiving tributaries from the hepatic, lumbar, gonadal, renal, and phrenic veins. The vessel then passes through the diaphragm at the level of T8, enters the pericardium, and drains into the lower portion of the right atrium.
The Chambers of the Heart
The heart is composed of four chambers: two atria and two ventricles.
- Blood returning to the heart first enters the atria before being transferred into the ventricles.
- From the left ventricle, blood is ejected into the aorta and distributed through the systemic circulation.
- From the right ventricle, blood is pumped into the pulmonary circulation via the pulmonary arteries.
This article examines the anatomy of the cardiac chambers, focusing on their positions, internal features, and relevant clinical correlations.
Atria
Right Atrium
The right atrium receives deoxygenated blood from the superior vena cava, inferior vena cava, and the coronary veins. Blood is then directed through the right atrioventricular orifice, which is guarded by the tricuspid valve, into the right ventricle.
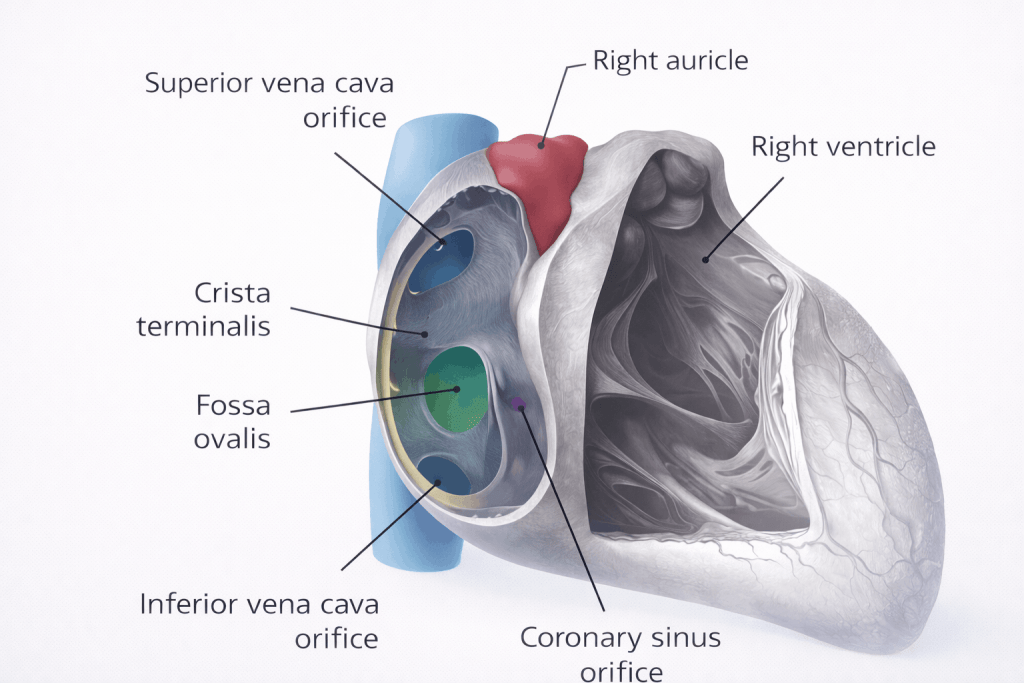
In the anatomical position, the right atrium forms the right border of the heart. Projecting from its anteromedial aspect is the right auricle (right atrial appendage), a muscular pouch that increases atrial capacity.
The internal surface of the right atrium is divided into two regions with distinct embryological origins, separated by a muscular ridge known as the crista terminalis:
- Sinus venarum: Located posterior to the crista terminalis, this smooth-walled region receives blood from the superior and inferior vena cavae and is derived from the embryonic sinus venosus.
- Atrium proper: Situated anterior to the crista terminalis and including the right auricle, this region has a rough, muscular surface formed by pectinate muscles and originates from the primitive atrium.
The coronary sinus, which drains venous blood from the myocardium, opens into the right atrium between the orifice of the inferior vena cava and the right atrioventricular orifice.
Interatrial Septum
The interatrial septum is a muscular partition separating the right and left atria.
On the septal wall of the right atrium is an oval depression called the fossa ovalis, which represents the remnant of the fetal foramen ovale. In fetal life, this opening allows blood to pass from the right atrium to the left, bypassing the lungs. It normally closes shortly after birth when pulmonary circulation is established.
Copyright medicpass.co.uk
Fig 1 – The right atrium and interatrial septum, with part of the atrium proper visible.
Clinical Relevance
Atrial Septal Defect
An atrial septal defect (ASD) is a persistent opening in the interatrial septum after birth. The most common form is a patent foramen ovale.
In adults, left atrial pressure is typically higher than right atrial pressure, resulting in a left-to-right shunt through the defect. Large defects can overload the right ventricle, leading to pulmonary hypertension, right ventricular hypertrophy, and eventual right-sided heart failure.
Definitive management involves closure of the defect, either surgically or via a transcatheter approach.
Left Atrium
The left atrium receives oxygenated blood from the four pulmonary veins and pumps it through the left atrioventricular orifice, guarded by the mitral valve, into the left ventricle.
Anatomically, the left atrium forms the posterior aspect (base) of the heart. The left auricle extends from the superior portion of the chamber and overlaps the root of the pulmonary trunk.
The internal surface of the left atrium is also divided into two embryologically distinct regions:
- Inflow portion: Receives blood from the pulmonary veins and has smooth walls; it develops from the pulmonary veins themselves.
- Outflow portion: Located anteriorly and including the left auricle; it contains pectinate muscles and is derived from the primitive atrium.
Ventricles
The ventricles receive blood from the atria and eject it into the great arteries: the aorta from the left ventricle and the pulmonary artery from the right ventricle.
Right Ventricle
The right ventricle receives deoxygenated blood from the right atrium and pumps it through the pulmonary orifice, guarded by the pulmonary valve, into the pulmonary artery.
It has a triangular shape and forms most of the anterior surface of the heart. The chamber is divided into an inflow and an outflow region, separated by a muscular ridge called the supraventricular crest.
Inflow Portion
The inner surface of the inflow region is covered by irregular muscular ridges known as trabeculae carneae, giving the ventricle a spongy appearance. These can be classified into three types:
- Ridges: Attached along their length to the ventricular wall
- Bridges: Attached at both ends but free in the middle; the most important example is the moderator band, which spans from the interventricular septum to the anterior ventricular wall and carries part of the right bundle branch of the conduction system
- Papillary muscles: Conical muscles anchored to the ventricular wall; their apices attach to the tricuspid valve cusps via chordae tendineae, preventing valve prolapse during systole
Outflow Portion (Conus Arteriosus)
The outflow tract of the right ventricle is located superiorly and leads to the pulmonary artery. It is derived from the embryonic bulbus cordis and has smooth walls, lacking trabeculae carneae.
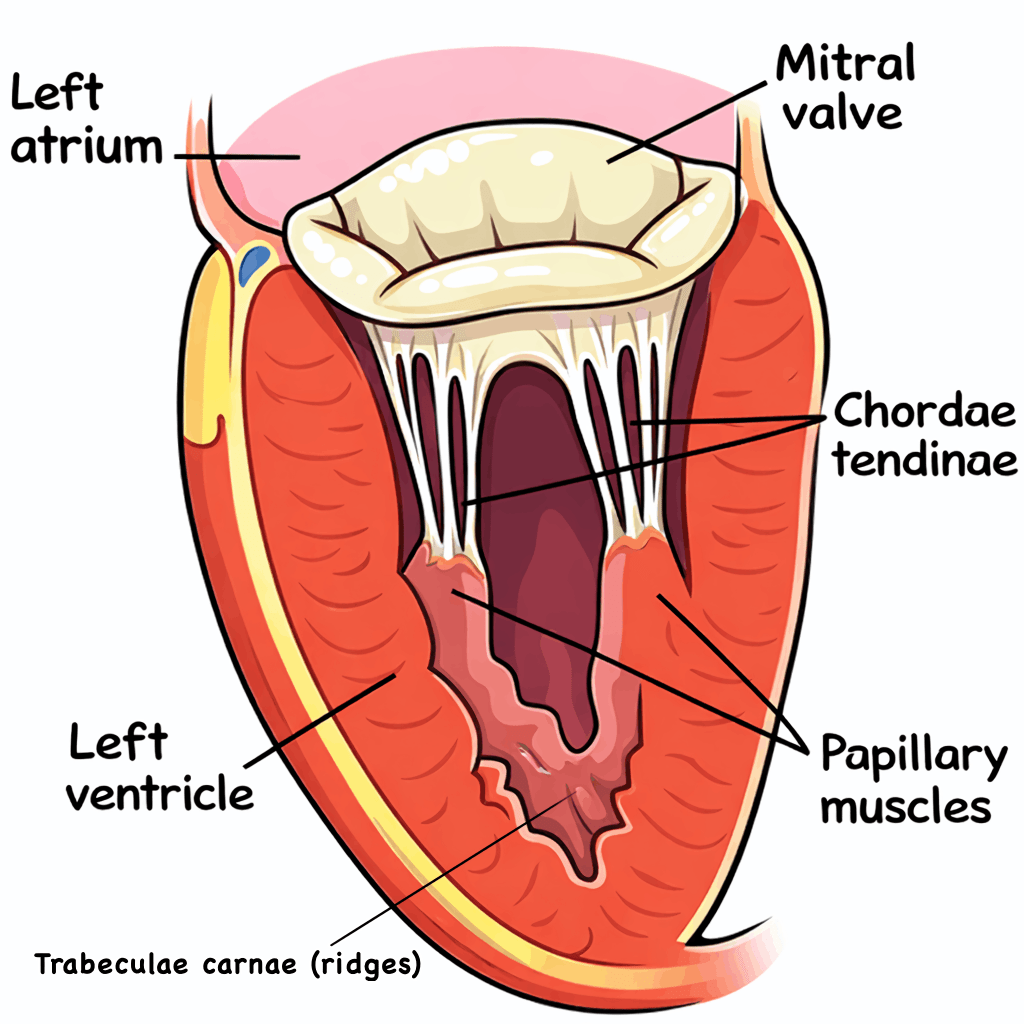
Fig 2 – Frontal section of the heart showing papillary muscle attachments to the atrioventricular valves.
Interventricular Septum
The interventricular septum separates the right and left ventricles and consists of two parts:
- Muscular part: Forms the majority of the septum and is similar in thickness to the left ventricular wall
- Membranous part: Thinner and contributes to the fibrous skeleton of the heart
Left Ventricle
The left ventricle receives oxygenated blood from the left atrium and ejects it through the aortic orifice, guarded by the aortic valve, into the aorta.
In the anatomical position, the left ventricle forms the apex of the heart, as well as the left and diaphragmatic surfaces. Like the right ventricle, it is divided into inflow and outflow regions.
Inflow Portion
The inflow region is lined with trabeculae carneae. Two papillary muscles are present, and their chordae tendineae attach to the cusps of the mitral valve.
Outflow Portion
The outflow tract, known as the aortic vestibule, has smooth walls without trabeculae carneae and is derived from the embryonic bulbus cordis.
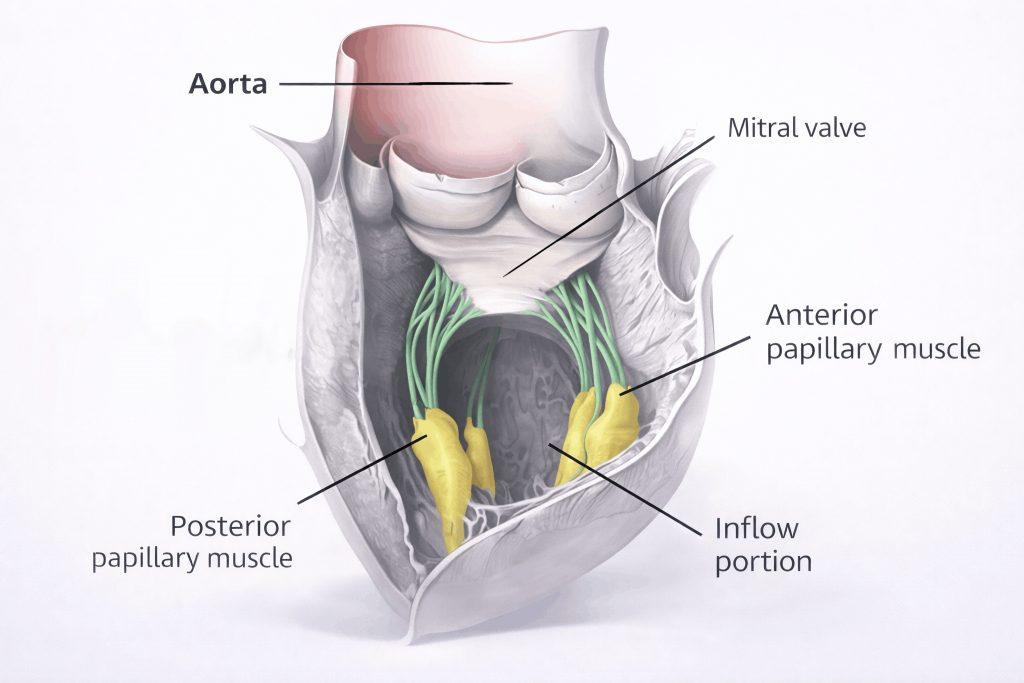
Fig 3 – Papillary muscles and inflow region of the left ventricle.
Clinical Relevance
Tetralogy of Fallot
Tetralogy of Fallot is a cyanotic congenital heart condition caused by a single developmental abnormality, resulting in four structural defects:
- Ventricular septal defect
- Overriding aorta (positioned directly above the ventricular septal defect)
- Pulmonary valve stenosis
- Right ventricular hypertrophy
Pulmonary valve stenosis increases resistance to outflow from the right ventricle, leading to hypertrophy. As right ventricular pressure rises above left ventricular pressure, blood is shunted from right to left through the ventricular septal defect. Because the aorta overrides the defect, deoxygenated blood enters the systemic circulation.
Treatment is typically surgical and is usually performed in early infancy, or shortly after birth in severe cases.
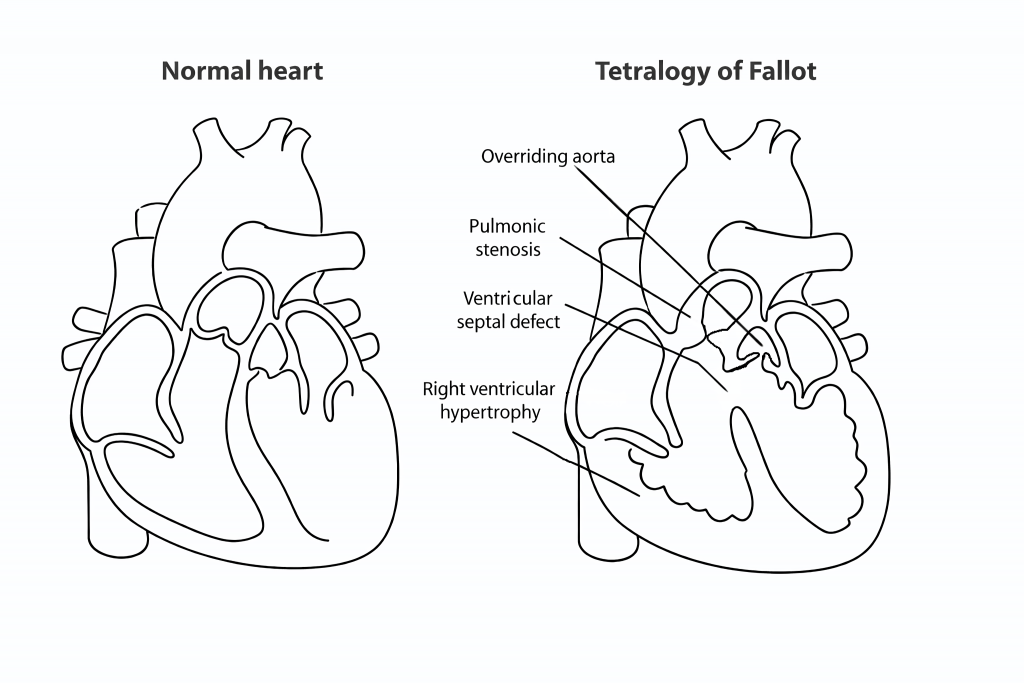
Fig 4 – Diagram showing the four anatomical abnormalities seen in Tetralogy of Fallot.
The Conducting System of the Heart
Contents
The cardiac conduction system is a network of specialised cells and nodes responsible for initiating and coordinating contraction of the heart muscle. It is made up of the following components:
- Sinoatrial node
- Atrioventricular node
- Atrioventricular bundle (bundle of His)
- Purkinje fibres
This article explores the anatomy of the cardiac conduction system, including its structure, function, and clinical significance.
Overview of Cardiac Conduction
A single cardiac cycle involves a specific sequence of electrical events:
- An electrical impulse (action potential) is generated by the sinoatrial (SA) node.
- This impulse spreads across the atrial myocardium, resulting in atrial contraction.
- When the signal reaches the atrioventricular (AV) node, it is briefly delayed.
- The impulse is then transmitted into the bundle of His and conducted down the interventricular septum.
- The bundle of His and Purkinje fibres distribute the impulse throughout the ventricles, triggering ventricular contraction.
The individual components of this system are described in more detail below.
Fig 1 – Illustration showing the spread of electrical conduction through the heart.
Components of the Cardiac Conduction System
Sinoatrial Node
The sinoatrial (SA) node is a cluster of specialised pacemaker cells located in the upper wall of the right atrium, near the point where the superior vena cava enters the chamber.
These cells are capable of spontaneous depolarisation, generating electrical impulses without external stimulation. The impulse produced by the SA node spreads through gap junctions across both atria, leading to atrial systole and movement of blood into the ventricles.
The firing rate of the SA node is regulated by the autonomic nervous system:
- Sympathetic stimulation increases the rate of impulse generation, raising heart rate.
- Parasympathetic stimulation reduces impulse frequency, lowering heart rate.
Atrioventricular Node
Following atrial conduction, electrical impulses converge at the atrioventricular (AV) node. This structure is located within the atrioventricular septum, close to the opening of the coronary sinus.
The AV node introduces a delay of approximately 120 milliseconds. This pause ensures that the atria have sufficient time to complete ventricular filling before ventricular contraction begins.
After this delay, the impulse is passed into the atrioventricular bundle.
Atrioventricular Bundle
The atrioventricular bundle, also known as the bundle of His, is a continuation of specialised conducting tissue from the AV node. Its role is to transmit electrical impulses from the atria to the ventricles.
It descends through the membranous portion of the interventricular septum and then divides into two branches:
- Right bundle branch – conducts impulses to the Purkinje fibres of the right ventricle
- Left bundle branch – conducts impulses to the Purkinje fibres of the left ventricle
Fig 2 – Overview of the components of the cardiac conduction pathway.
Purkinje Fibres
The Purkinje fibres form a subendocardial network of specialised conduction cells. They are rich in glycogen and connected by numerous gap junctions, enabling rapid transmission of electrical signals.
Located along the inner surfaces of the ventricular walls, these fibres rapidly convey impulses from the atrioventricular bundle to the ventricular myocardium. This fast conduction ensures coordinated ventricular systole, allowing blood to be efficiently ejected from the right ventricle into the pulmonary artery and from the left ventricle into the aorta.
Clinical Relevance
Artificial Pacemaker
An artificial pacemaker is a small electronic device used to monitor and regulate heart rhythm. It is typically implanted beneath the left clavicle, with leads threaded through the venous system into the heart.
The most common indication for pacemaker implantation is bradycardia. The device continuously monitors heart rate and delivers electrical impulses only when the rate falls below a set threshold. Pacemakers may also be used in the management of certain tachyarrhythmias, heart block, and other conduction abnormalities.
Fig 3 – Illustration of the cardiac conduction system and examples of pacemaker types, including single- and dual-chamber devices.
The Coronary Circulation
Written by Sophie Stanley
Contents
All tissues in the body require a continuous supply of oxygen and nutrients, and the heart itself is no exception. The coronary circulation refers to the network of blood vessels responsible for supplying and draining the myocardium. The coronary arteries are so named because they encircle the heart in a crown-like pattern.
This article describes the naming conventions, anatomical distribution, and clinical importance of the vessels that make up the coronary circulation.
Naming
Coronary Arteries
Two principal arteries supply the heart: the right coronary artery (RCA) and the left coronary artery (LCA). Both arise from the right and left aortic sinuses of the ascending aorta.
The aortic sinuses are small dilations located just above the cusps of the aortic valve. When the heart relaxes during diastole, blood flows back toward the valve, filling these sinuses and allowing blood to enter the coronary arteries.
The left coronary artery quickly divides into major branches. Its most prominent branch is the left anterior descending artery (LAD), also known as the anterior interventricular artery. The LCA also gives rise to the left circumflex artery (Cx) and the left marginal artery (LMA). In approximately 20–25% of individuals, the circumflex artery continues posteriorly to form the posterior interventricular artery (PIv).
The right coronary artery gives rise anteriorly to the right marginal artery (RMA). In the majority of people (around 80–85%), the RCA also forms the posterior interventricular artery on the posterior surface of the heart.
Cardiac Veins
Venous blood from the heart is drained mainly by the coronary sinus, a large venous channel located on the posterior aspect of the heart. The coronary sinus empties directly into the right atrium. In addition, several smaller cardiac veins drain directly into the right atrium.
The main tributaries of the coronary sinus include:
- Great cardiac vein (anterior interventricular vein): The largest tributary. It begins at the apex of the heart, ascends in the anterior interventricular groove, curves to the left, and continues onto the posterior surface where it enlarges to form the coronary sinus.
- Small cardiac vein: Runs in the groove between the right atrium and right ventricle on the anterior surface, then continues posteriorly to drain into the coronary sinus.
- Middle cardiac vein (posterior interventricular vein): Arises at the apex and ascends in the posterior interventricular groove to enter the coronary sinus.
- Posterior cardiac vein: Located on the posterior surface of the left ventricle, lying to the left of the middle cardiac vein, and draining into the coronary sinus.
Distribution of the Coronary Arteries
In general, a coronary artery supplies the region of myocardium over which it travels. The anatomical courses of the main coronary arteries are outlined below.
The right coronary artery passes to the right of the pulmonary trunk and runs within the coronary (atrioventricular) sulcus. The right marginal artery branches from it and descends along the right and inferior border of the heart toward the apex. The RCA continues around to the posterior surface, still within the coronary sulcus, where it commonly gives rise to the posterior interventricular artery, which runs toward the apex in the posterior interventricular groove.
The left coronary artery passes between the pulmonary trunk and the left auricle before dividing into the anterior interventricular (LAD) and circumflex branches. The LAD runs within the anterior interventricular groove toward the apex and often continues onto the posterior surface to anastomose with the posterior interventricular artery. The circumflex artery follows the coronary sulcus to the left border of the heart and onto its posterior surface, giving rise to the left marginal branch along the left border.
Clinical Relevance
Coronary Artery Disease
Coronary artery disease (CAD), also known as coronary heart disease, is one of the leading causes of death in the UK and worldwide. It is characterised by reduced blood flow to the myocardium.
Reduced coronary perfusion most commonly results from narrowing or obstruction of the coronary arteries. Causes include atherosclerosis, thrombosis, hypertension, diabetes, and smoking. These factors impair blood flow through either physical blockage or pathological changes in the vessel wall.
One common manifestation of CAD is angina pectoris, which presents as transient chest pain during exertion. This occurs because the oxygen supply to the myocardium is insufficient to meet increased demand. The pain typically resolves with rest. Angina is exercise-related because coronary arteries fill primarily during diastole; during exercise, the diastolic phase shortens, leaving less time for blood to pass through narrowed vessels.
If untreated, angina may progress to myocardial infarction (MI). Acute occlusion of a coronary artery leads to infarction and necrosis of the myocardium supplied by that vessel. The affected region of the heart depends on which artery is blocked. Changes on an ECG can help localise the site of infarction:
| Description | ECG leads affected | Artery involved |
|---|---|---|
| Inferior | II, III, aVF | RCA |
| Anteroapical | V3, V4 | Distal LAD |
| Anteroseptal | V1, V2 | LAD |
| Anterolateral | I, aVL, V5, V6 | Circumflex |
| Extensive anterior | I, aVL, V2–V6 | Proximal LCA |
| True posterior | Tall R wave in V1 | RCA |
Diagnosis and Treatment of Coronary Artery Disease
Significant coronary artery blockages can be identified using a coronary angiogram. This procedure involves advancing a catheter into the aorta via the femoral artery, injecting contrast dye into the coronary arteries, and visualising them with X-ray imaging.
Immediate treatment may involve coronary angioplasty, in which a balloon is inflated within the narrowed segment of the artery to compress atherosclerotic plaque and restore blood flow. An intravascular stent is often placed to keep the artery open and maintain adequate perfusion.
Appendix A – Overview of the Coronary Vasculature
| Artery | Region Supplied | Vein Draining Region |
|---|---|---|
| Right coronary artery | Right atrium, SA and AV nodes, posterior third of interventricular septum | Small cardiac vein, middle cardiac vein |
| Right marginal artery | Right ventricle, apex | Small cardiac vein, middle cardiac vein |
| Posterior interventricular artery | Right and left ventricles, posterior third of IVS | Left posterior ventricular vein |
| Left coronary artery | Left atrium, left ventricle, interventricular septum, AV bundle | Great cardiac vein |
| Left anterior descending artery | Right and left ventricles, anterior two-thirds of IVS | Great cardiac vein |
| Left marginal artery | Left ventricle | Left marginal vein, great cardiac vein |
| Circumflex artery | Left atrium, left ventricle | Great cardiac vein |
The Heart Wall
Contents
- Endocardium
- Endocarditis
- Myocardium
- Myocarditis
- Epicardium
The wall of the heart is made up of three distinct layers:
- Endocardium (innermost layer)
- Myocardium (middle muscular layer)
- Epicardium (outermost layer)
Each layer has a specific structure and role, and disease affecting any of them can result in significant cardiovascular pathology.
This article reviews the anatomy of the heart wall layers and highlights their clinical relevance.
Endocardium
The endocardium forms the inner lining of the heart, covering the chambers and heart valves.
It is composed of simple squamous epithelium supported by loose connective tissue and closely resembles the endothelial lining of blood vessels.
In addition to providing a smooth surface that facilitates efficient blood flow, the endocardium contributes to cardiac development and helps regulate myocardial contraction.
Subendocardial Layer
The subendocardial layer is a thin zone of loose connective tissue situated between the endocardium and myocardium.
This layer is clinically important as it contains the Purkinje fibres and other elements of the cardiac conduction system.
Because the conduction pathways run within this layer, injury or ischaemia affecting it can disrupt electrical signalling and lead to cardiac arrhythmias.
Fig 1 – The layers of the heart wall.
Clinical Relevance
Endocarditis
Endocarditis is inflammation of the endocardium, most often involving the heart valves.
It is usually caused by bacterial infection and leads to the formation of vegetations, which are aggregates of platelets, fibrin, microorganisms, and inflammatory cells on valve surfaces.
These changes can damage valves, produce cardiac murmurs, and increase susceptibility to recurrent infection. Without treatment, endocarditis may result in serious complications such as heart failure or embolic events.
Myocardium
The myocardium constitutes the majority of the heart wall and is made up of involuntary, striated cardiac muscle.
It is the main contractile layer of the heart, generating the force required to pump blood through the pulmonary and systemic circulations.
Subepicardial Layer
Located between the myocardium and epicardium, the subepicardial layer contains coronary blood vessels, nerves, and connective tissue.
Clinical Relevance
Myocarditis
Myocarditis is inflammation of the myocardium, most commonly caused by viral infections such as coxsackie B virus. Typical symptoms include chest pain, palpitations, and breathlessness.
Inflammation can directly impair myocardial contractility, reducing cardiac output. As a result, myocarditis may lead to arrhythmias, dilated cardiomyopathy, and eventually heart failure.
Epicardium
The epicardium is the outermost layer of the heart wall and corresponds to the visceral layer of the serous pericardium.
It consists of loose connective tissue and adipose tissue, covered externally by a layer of simple squamous epithelial cells known as mesothelium.
Key functions of the epicardium include:
- Acting as a protective outer covering of the heart
- Secreting pericardial fluid to lubricate the heart within the pericardial cavity
- Minimising friction during cardiac movement and contraction
The Pericardium
Contents
Anatomical Structure
Transverse Pericardial Sinus
Innervation
If the heart is likened to the soft, functional interior of an orange, the pericardium can be compared to the peel that surrounds it. While it may appear less interesting at first glance, the pericardium performs several vital physiological roles.
In anatomical terms, the pericardium is a fibroserous, fluid-filled sac that encloses the muscular heart and the proximal portions of the great vessels, including the aorta, pulmonary artery, pulmonary veins, and the superior and inferior vena cavae.
This article provides an overview of the pericardium, focusing on its structure, function, innervation, and clinical importance.
Anatomical Structure
The pericardium consists of two principal layers: a strong outer fibrous pericardium and a thin inner serous pericardium.
Fibrous Pericardium
The fibrous pericardium is composed of dense connective tissue and is continuous inferiorly with the central tendon of the diaphragm. It is relatively non-distensible, a feature that helps prevent sudden overexpansion of the heart. However, this rigidity can also contribute to serious clinical conditions, such as cardiac tamponade.
Serous Pericardium
Contained within the fibrous pericardium, the serous pericardium is divided into two layers:
- Parietal layer – lines the inner surface of the fibrous pericardium
- Visceral layer – adheres to the surface of the heart and forms its outermost layer, also known as the epicardium
Both layers consist of a single layer of mesothelial cells. Between them lies the pericardial cavity, which contains a small volume of serous fluid. This fluid reduces friction as the heart moves and contracts.
Fig 1 – Layers of the heart wall.
A helpful way to remember the order of the pericardial layers is the mnemonic “Fart Police Smell Villains”:
- F – Fibrous pericardium
- P – Parietal layer of serous pericardium
- S – Serous fluid
- V – Visceral layer of serous pericardium
Functions
The pericardium performs several important physiological functions:
- Stabilisation of the heart: It anchors the heart within the mediastinum and limits excessive movement. This fixation is achieved through attachments to the diaphragm, sternum, and the outer layers of the great vessels.
- Prevention of overfilling: The inelastic fibrous pericardium restricts rapid cardiac dilation, placing a physical limit on heart size.
- Lubrication: Serous fluid between the layers of the serous pericardium reduces friction during cardiac motion.
- Protection from infection: The fibrous pericardium acts as a barrier between the heart and neighbouring structures, such as the lungs, which are more susceptible to infection.
Fig 2 – Anterior view of the pericardium showing its attachments to the diaphragm and great vessels.
Clinical Relevance
Transverse Pericardial Sinus
The transverse pericardial sinus is a short channel within the pericardial cavity that forms during embryological folding of the heart tube.
It is positioned:
- Posterior to the ascending aorta and pulmonary trunk
- Anterior to the superior vena cava
This arrangement separates the arterial outflow of the heart (aorta and pulmonary trunk) from the venous inflow (superior vena cava and pulmonary veins).
The transverse sinus is clinically significant during coronary artery bypass grafting (CABG), as it allows surgeons to place a clamp or ligature around the ascending aorta and pulmonary trunk.
Fig 3 – Diagram of the transverse pericardial sinus and its anatomical relationships.
Innervation
The pericardium receives somatic sensory innervation from the phrenic nerves (C3–C5), which also innervate the diaphragm.
Because these nerves originate in the cervical region, irritation of the pericardium—such as in pericarditis—may cause referred pain to the shoulder.
Clinical Relevance
Cardiac Tamponade
The fibrous pericardium’s limited ability to stretch becomes problematic when excess fluid accumulates in the pericardial cavity, a condition known as pericardial effusion.
As pressure within the pericardial sac increases, the heart chambers can become compressed, impairing filling and reducing cardiac output. This life-threatening situation is referred to as cardiac tamponade.
Pericarditis
Pericarditis is inflammation of the pericardium and can arise from various causes, including infection and myocardial infarction. It commonly presents with chest pain and may progress to cardiac tamponade if fluid accumulates rapidly in the pericardial cavity.
Fig 4 – Chest radiograph demonstrating an enlarged cardiac silhouette due to pericardial effusion.
¹ The remarkable properties of orange peel are well documented in scientific literature—for example, the oils extracted from orange peel are highly flammable.
The Surfaces and Borders of the Heart
Contents
Orientation and Surfaces
Borders
Sulci of the Heart
Pericardial Sinuses
Transverse Pericardial Sinus
The heart is a hollow, muscular organ that functions as a pump and is situated within the middle mediastinum.
It has a complex, pyramid-like form with multiple distinct surfaces and borders. Shallow grooves on its exterior, known as sulci, mark important internal divisions.
This article reviews the orientation of the heart, along with its surfaces and borders.
Orientation and Surfaces
The heart can be visualised as a pyramid that has tipped forward, with its apex directed anteroinferiorly.
When viewed in the anatomical position, the heart has five surfaces, each primarily formed by specific chambers:
- Anterior (sternocostal) surface – formed mainly by the right ventricle
- Posterior surface (base of the pyramid) – formed largely by the left atrium
- Inferior (diaphragmatic) surface – formed by both the left and right ventricles
- Right pulmonary surface – formed by the right atrium
- Left pulmonary surface – formed by the left ventricle
Borders
The borders of the heart lie between its surfaces and help define its overall shape. There are four principal borders:
- Right border – formed by the right atrium
- Inferior border – formed by the right and left ventricles
- Left border – formed mainly by the left ventricle, with a small contribution from the left atrium
- Superior border – formed by the right and left atria and the great vessels
Fig 1 – Anatomical illustration showing the borders of the heart.
Sulci of the Heart
Internally, the heart is divided into four chambers. These internal separations are reflected externally as grooves called sulci.
There are three main sulci:
- Coronary sulcus (atrioventricular groove): Encircles the heart and marks the division between the atria and ventricles. It contains the right coronary artery, the circumflex branch of the left coronary artery, the small cardiac vein, and the coronary sinus.
- Anterior interventricular sulcus: Located on the anterior surface and separates the left and right ventricles. It contains the anterior interventricular artery (left anterior descending artery) and the great cardiac vein.
- Posterior interventricular sulcus: Found on the posterior surface and also separates the ventricles. It contains the posterior interventricular artery and the middle cardiac vein.
Pericardial Sinuses
Pericardial sinuses are not true anatomical sinuses like those found in the skull. Instead, they are recesses formed by the way the pericardium reflects around the great vessels.
- The oblique pericardial sinus is a blind-ending recess located on the posterior aspect of the heart.
- The transverse pericardial sinus lies superiorly and has important surgical significance, as outlined below.
Clinical Relevance
Transverse Pericardial Sinus
The transverse pericardial sinus is positioned:
- Posterior to the ascending aorta and pulmonary trunk
- Anterior to the superior vena cava
- Superior to the left atrium
In this location, it separates the arterial outflow vessels of the heart (the aorta and pulmonary trunk) from the venous inflow vessels (the superior vena cava and pulmonary veins).
This anatomical relationship is exploited during coronary artery bypass grafting, where the transverse pericardial sinus allows surgeons to identify and temporarily ligate the major arteries supplying the heart.
Fig 2 – Diagram demonstrating the transverse pericardial sinus and its relationship to the major arteries and veins of the heart.
The Valves of the Heart
Contents
Atrioventricular Valves
Semilunar Valves
Aortic Stenosis
The heart valves ensure that blood moves through the heart in a single, forward direction. They are formed from connective tissue and are lined by endocardium, the innermost layer of the heart wall.
There are four cardiac valves, grouped into two main types:
- Atrioventricular (AV) valves: the tricuspid valve and the mitral (bicuspid) valve. These sit between each atrium and its corresponding ventricle.
- Semilunar valves: the pulmonary valve and the aortic valve. These lie between the ventricles and their respective outflow arteries, controlling blood ejection from the heart.
This article reviews the anatomy of the heart valves, including their structure, function, and clinical significance.
Fig 1 – The four heart valves shown with the atria and great vessels removed.
Atrioventricular Valves
The atrioventricular valves are positioned between the atria and ventricles. They close at the onset of ventricular systole, producing the first heart sound. The two AV valves are:
- Tricuspid valve: Located between the right atrium and right ventricle at the right atrioventricular orifice. It has three cusps—anterior, posterior, and septal—each anchored at its base to a fibrous ring surrounding the valve opening.
- Mitral valve: Situated between the left atrium and left ventricle at the left atrioventricular orifice. It is also known as the bicuspid valve, as it has two cusps (anterior and posterior). Like the tricuspid valve, its cusps are secured to a fibrous annulus.
Both valves are stabilised by chordae tendineae, fibrous cords attached to the free edges of the valve cusps. These cords connect to papillary muscles on the ventricular walls. During ventricular contraction, the papillary muscles contract, preventing the valve leaflets from prolapsing back into the atria.
In total, there are five papillary muscles: three in the right ventricle supporting the tricuspid valve, and two in the left ventricle supporting the mitral valve.
Fig 2 – Papillary muscles and the inflow region of the left ventricle.
Semilunar Valves
The semilunar valves are located between the ventricles and their outflow vessels. They close at the start of ventricular diastole, generating the second heart sound. There are two semilunar valves:
- Pulmonary valve: Found between the right ventricle and the pulmonary trunk. It consists of three cusps—left, right, and anterior—named according to their fetal positions before cardiac rotation.
- Aortic valve: Located between the left ventricle and the ascending aorta. It also has three cusps—left, right, and posterior.
The left and right aortic sinuses give rise to the left and right coronary arteries. During ventricular relaxation, blood recoils into the aortic sinuses, allowing coronary blood flow to supply the myocardium.
Structurally, the pulmonary and aortic valves are very similar. Each cusp attaches along its sides to the wall of the outflow vessel, which is slightly expanded to form a sinus. The free upper edge of each cusp is thickened to form the lunule, with a central thickening called the nodule.
At the beginning of diastole, blood flows back toward the heart, filling the sinuses and forcing the cusps together, thereby closing the valve.
Fig 3 – Aortic valve cusps, aortic sinuses, and the origins of the coronary arteries.
Clinical Relevance
Aortic Stenosis
Aortic stenosis describes narrowing of the aortic valve, which restricts blood flow from the left ventricle into the aorta. The three most common causes are:
- Age-related calcification
- Congenital abnormalities, most commonly a bicuspid aortic valve, which predisposes the valve to later calcification
- Rheumatic fever
Severe aortic stenosis classically presents with a triad of symptoms: shortness of breath, syncope, and angina. The increased resistance to outflow also raises the workload of the left ventricle, often leading to left ventricular hypertrophy.
Definitive management is surgical and may involve valve replacement or balloon valvuloplasty.
Fig 4 – Aortic stenosis caused by rheumatic heart disease, showing thickened and fused valve cusps with the coronary artery openings visible from above.